

Spot reduction. Friend only to infomercial ab blasters, thigh creams, and fat stripper pills. In this article, exercise physiologist Dr Dan Jolley, PhD, reviews the scientific evidence on spot reduction and puts Charles Poliquin’s BioSignature Modulation claims under the microscope. Over to you Dr Dan. –Bill
During my many years as a personal trainer I quickly got used to hearing some of the same comments from clients, over and over.
Young men wanted to put on muscle, young women were scared of putting on too much muscle, and almost everyone wanted to lose body fat.
The latter was by far the most common, and it is this concern about body fat that has sprouted urban fitness myths that have survived and thrived for decades despite all attempts to correct them.
Almost every second client I started training would point to a specific part of their body (i.e., stomach, hips, thighs, arms, or butt) and tell me that was the area they needed to lose weight.
This idea is known as “spot reduction.”
The proposed mechanisms of spot reduction vary depending on who is selling the idea (or the product that purportedly promotes spot reduction), but the theme is consistent: exercise a specific part of your body, and you can lose weight from that part of the body.
Cycle for skinnier thighs, do arm exercises for skinnier arms, or hip movements for slimmer hips.
Edwin Checkley: The Godfather of Spot Reduction
The idea of spot reduction is nothing new. In fact, it’s old – really old.
In 1890 Edwin Checkley released a book called “A Natural Method of Physical Training.”
Chapter seven discusses obesity and makes what is possibly the first reference to spot reduction (though if you find an earlier one, let me know!).
Checkley makes the following claim:
“The dissipation of fat is local; that is to say, it disappears in localities in which muscles are active, and in proportion to their activity. Thus people will accumulate fat in accordance very largely with their personal habits. People who sit a great deal, yet have occasion to use their arms considerable, will be found with arms having proportionately more muscle and less fat than their legs.”
Intuitively this makes sense to us, which is why it has been such an enduring idea.
And until the advent of a rigorous scientific method and accurate body composition technologies, it was hard to disprove this.
But today we know a lot more about fat loss.
And tellingly, as our technology and measurement of body fat has improved, the evidence refuting this old theory has mounted up.
Body fat measurement techniques such as skinfolds (although early evidence was mixed), ultrasound, muscle biopsy, MRI, and the modern gold standard DEXA scans (and another reference for good measure here) have all shown that specific exercise does not result in site-specific fat loss. Somehow, the idea persists in spite of this mountain of evidence.
You only have to look at women’s magazines down at your local supermarket to see how the idea of spot reduction endures.
The covers are plastered with the promise of a flat stomach, lean butt, or toned arms.
The pages are loaded with series of exercises (probably low intensity body weight exercises) that work the body part in question.
And while it is entirely possible that this exercise program may work towards the desired effect, far more important are the dietary changes required for this desired weight loss effect (or the large amounts of energy expended during a cardio or heavy weights workout).
Yes, this sounds a lot harder. Yes, it takes longer. But it is unavoidable.
BioSignature Modulation and spot reduction
Given the scientific evidence against the existence of spot reduction, if it were to be taken seriously again, any new evidence would need to be overwhelming.
But a few years ago, a modern take on spot reduction idea emerged.
Unusual for this type of pseudoscience, it was from a far more reputable source than a women’s fitness magazine!
Charles Poliquin is a Canadian strength and conditioning coach, with a master’s degree in exercise physiology – much like myself (though not being a Canadian, I had to settle for marrying one!).
Poliquin used to be considered cutting edge. Some of his books and articles on resistance training were quite influential, as was his work on periodisation (here).
But I fear he may have “jumped the shark” a few years ago when he first promoted the idea of “Biosignature Modulation.”
He spent a lot of time promoting the concept and running workshops, before selling the brand in 2013 (now owned by the Poliquin Group).
Poliquin’s explanation of BioSignature Modulation begins with a description of his method of assessing body composition:
“There are 12 major body fat sites that can be quickly and accurately tested by a pair of quality skin calipers and a qualified technician… I believe that body fat testing with skin calipers is the best method to be used for Biosignature Modulation because it can determine precisely the amount of fat in each of the major fat-testing sites were [sic] other testing methods only tell you your percent body fat.”
Sounds great, but here’s the problem.
There are some pretty well-known issues with skinfold measurement, particularly in the fitness industry.
First, skinfold-thickness equations frequently used by clinicians and practitioners have been shown to underestimate percent body fat.
Second, skinfold testing may not be sensitive enough to detect small changes in body fat.
This means a person might think nothing’s happened from their diet and exercise when in fact there were positive changes in body composition.
Third, tester error is a common problem with skinfolds.
Trainers get very basic instruction in skinfold measurement as part of their Certificate III in Fitness course, and the variation in technique and measurement is far greater than what you would see in a specialised course (such as an ISAK Level 1 course).
Fourth, not all personal trainers may have access to top quality skinfold calipers, which may cost around $400-500 and must be calibrated every 12 months.
Even if skinfold measurements are done accurately, there are still issues in assessing obese clients – and visceral fat (deep fat inside the abdominal cavity) isn’t assessed at all.
Triceps skinfold measurements
Once we’ve gathered skinfold measurements, then what happens?
Well, Poliquin says we need to interpret our results this way:
“Measurements from each site are then compared to the triceps reading and this identifies which areas of the body have excessive levels of fat relative to the other 11 body fat sites. Some people may have excessive fat in just one area, while others may have several problem areas.”
Hopefully you can see the problem here straight away.
Why are we comparing everything else to the triceps measurement? Poliquin does not explain this.
What happens if your triceps measurement is high? This impacts all our comparisons!
For example, if someone has a triceps measurement of 5 mm and a mid-thigh measurement of 25 mm, the ratio of these two measurements is 1:5.
For the sake of the argument, let’s say that 1:3 is an acceptable triceps to mid-thigh ratio.
If the triceps measurement was 10 mm and the mid-thigh was 28 mm then, relatively speaking, this person has an “acceptable” ratio of 1:2.8.
In the second example, the person with a higher skinfold total would appear to fare better in terms of ratio despite having more fat than in the first example.
I have no idea what the actual cut-offs for the numbers should be according to BioSignature Modulation, as I was not able to find any scientific validation, explanation, or justification for this.
Hormones and spot reduction
The next step is the most concerning for me. BioSignature Modulation suggests that specific hormones are responsible for body fat in certain sites and should be controlled through a combination of diet, exercise, and supplementation.
A screenshot of the summary (complete with the author’s spelling errors) is below:
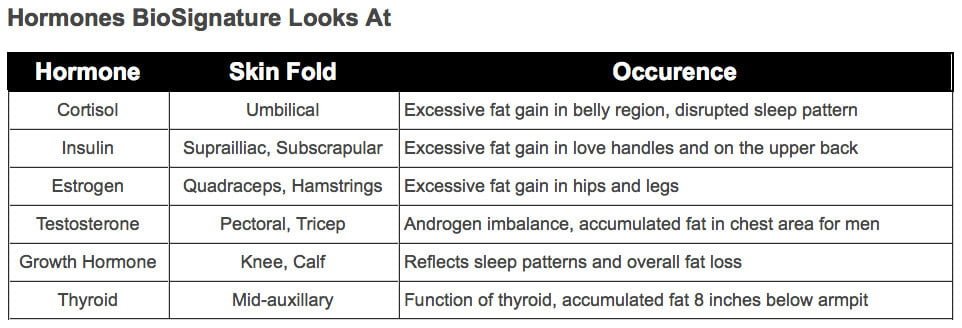
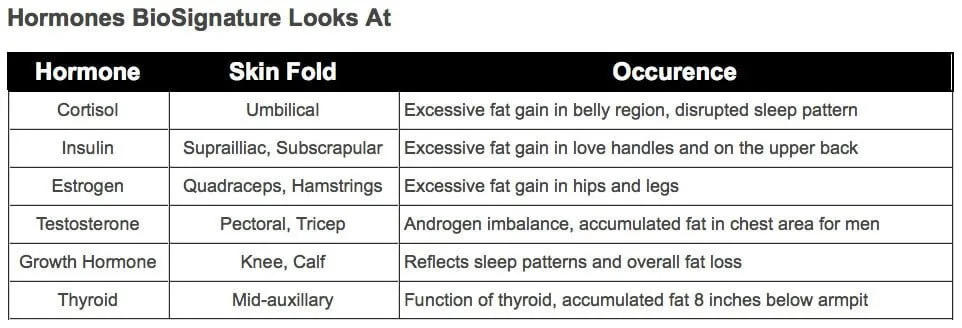
I agree that a healthy lifestyle is important for controlling body fat.
But my concern with this table is that it’s an oversimplified explanation of the individual effects of hormones on regional body composition.
In reality, we know that bodies come in all sizes and shapes due to inter-individual variations in genetics, gender, diets, lifestyle habits, gut microbiota, hormone to hormone interactions, neurotransmitters, effects of medications, etc.
Trying to whittle it all down into a simple “this hormone equals this body shape” is naive and misinformed.
Here is a more thorough review on BioSignature Modulation, hormones, and the program’s limitations which you might find interesting.
Diagnosing clients’ hormonal imbalances?
The above table also calls scope of practice into question. According to the BioSignature website, Poliquin explicitly states:
“Let’s say that after being tested, it’s discovered that there is an excessive amount of fat on the lower thighs (again, relative to the other major fat sites). This indicates that there is a problem with the estrogen levels. If the problem area is the triceps, the issue is with the androgen levels. If the problem area is the shoulder blades or hip, the problem is with your insulin levels.”
If this isn’t diagnosing clients (i.e., practicing medicine without a license?) then I don’t know what you call it.
You can see for yourself that a trainer learning BioSignature Modulation might be inclined to make assumptions about a client’s hormone levels by relying on such information.
This can create unwarranted fear and anxiety in clients that may already be dealing with other physical or mental issues.
Understanding correlation vs cause and effect
Even a cursory look through the research will provide plenty of reading about a correlation between high levels of abdominal body fat (and specifically a high waist-to-hip ratio) and high insulin levels.
This is because higher body fat levels are associated with reduced insulin sensitivity and an increased risk of developing type 2 diabetes (further reading here)
Body fat in the trunk has been shown to have a greater effect on insulin sensitivity than fat in the extremities, but this refers to all body fat in the trunk, not just around the shoulder blade.
Poliquin then suggests that “controlling blood sugar levels of the body with more frequent meals, reduced daily carbohydrate and low GI [glycaemic index] food choices is critical.”
Low GI food choices do not influence weight loss anywhere near as much as energy restriction does, so it is implausible to suggest that this will lead to selective and preferential body fat reduction in the upper back.
Some may be fooled when their upper body skinfolds do, in fact, decrease.
But if there is a general decrease in body fat as a result of increased exercise and healthier eating, skinfolds will change all over the body.
It is not appropriate to assume that just because a person’s insulin levels decrease, and their skinfolds decrease, that there is a direct causal link between the two.
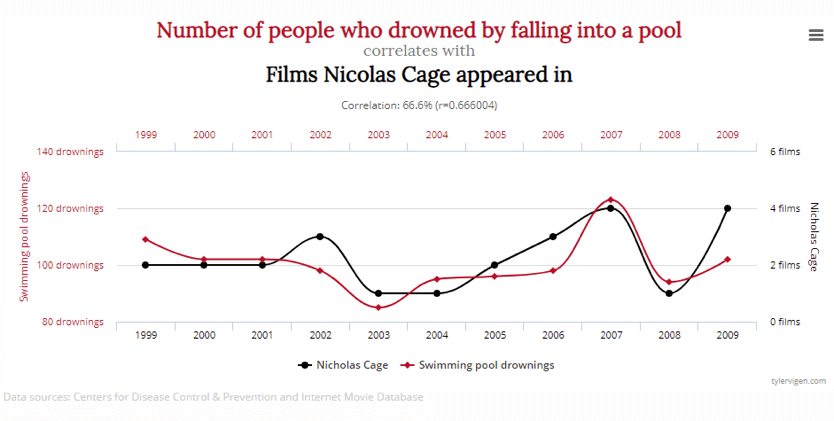
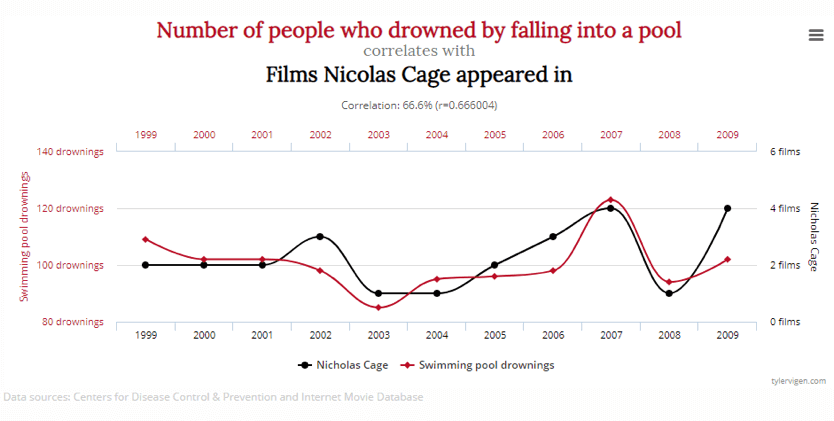
If you’re a trainer, memorise this: Correlation does NOT always mean cause and effect! Check out this site on spurious correlations and you’ll get a clear picture of what I mean.
BioSignature Modulation and supplementation
Poliquin also recommends supplements for spot reduction. He writes:
“For the fat stored around the shoulder blade… corosolic acid, alpha lipoic acid and fish oils may be prescribed to control insulin.”
We’ve already established that controlling insulin will not preferentially reduce body fat in the upper back.
But if it did, the evidence is preliminary at best.
Corosolic acid, for example, has been found to have an effect in mice, petri dishes, and some human trials, though many papers appear in alternative medicine journals, rather than more reputable titles.
And while early results in humans have shown some promise, with closer examination and better designed research, these early positive results tend to disappear.
In the meantime, though, you can very conveniently find a number of supplements in the Poliquin Group’s online store.
Scientific evidence for BioSignature Modulation?
So given the faulty logic and patchy evidence I’ve outlined so far, what is Poliquin’s evidence for his controversial spot reduction theory? In his own words:
“Biosignature Modulation is a scientific approach to [sic] spot reduction that I have developed over 20 years of performing blood, urine and saliva tests while working with world record holders, professional athletes in all the major sports, and Olympic medalists in sixteen different events.”
The problem with this is that research findings can only be reliably applied to the population upon which the testing was conducted.
So research conducted on elite level athletes can inform the training and nutrition of similar athletes, but not necessarily the rest of the population (i.e., your client trying to lose a few kilos of body fat).
Similarly, the differences between athletes and training methods of various sports and disciplines make it impossible to assume that research can be applied to all of them without a lot of follow-up research – research which, in this case, has not been done.
Another concern is that this type of evidence is generally described as “case studies.”
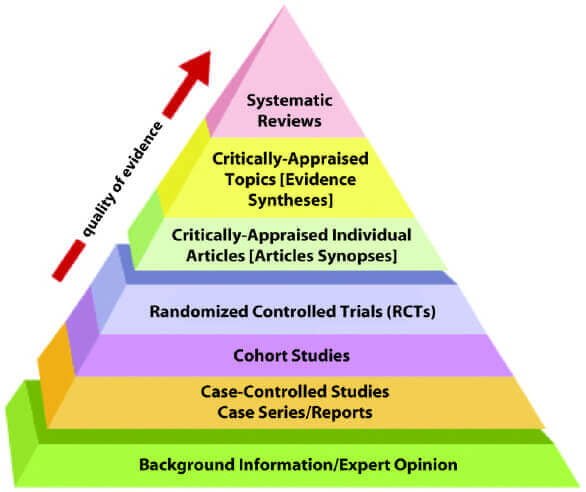
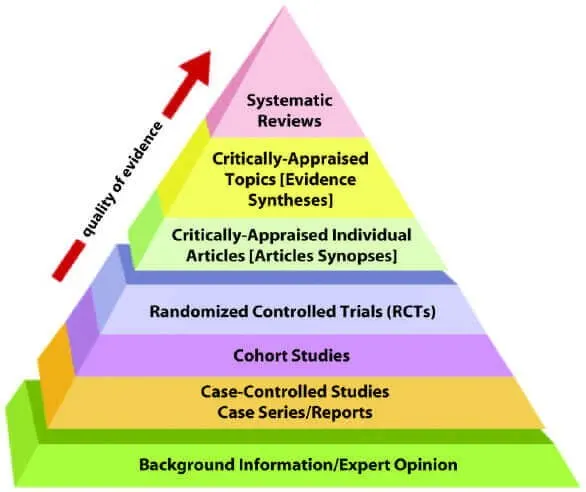
This is a nice way of saying “anecdote” – not the strongest form of research as you’ll see in the image below.
Evidence can come in many different forms, depending on what it is you are trying to test.
Case studies are generally considered pretty poor evidence, as it is impossible to control for other variables.
When someone loses weight, we need to consider not only diet and exercise factors, but also their psychological state, support from friends and family, the quality of their sleep, stress, and other factors that may change compliance to their healthy lifestyle habits.
Two case studies are not necessarily any better than one, because the factors influencing each may be completely different, meaning you can’t reliably compare the two.
Similarly, twenty case studies are not any better than two.
On the other hand, if you were to take these twenty people, put them on identical programs, and control other variables as much as you can, then we’re getting somewhere.
Poliquin didn’t do this though.
He tells us about a series of case studies on a unique population, doesn’t publicly provide the results, then applies his theory to the general population.
For BioSignature Modulation to have any scientific street cred, Poliquin would need to not only conduct strictly controlled studies but he would need to submit his results to reputable journals where they would undergo review by highly-qualified experts related to the subject matter (i.e., endocrinology).
After a series of revisions, a decision would be made on whether or not his research cut the mustard and is worthy of publication in a peer-reviewed medical journal.
Scope of Practice
All the aforementioned limitations of Poliquin’s ideas aside, there is another equally pressing concern: scope of practice.
I know I addressed this briefly above, but it warrants further discussion here.
The BioSignature Modulation course required to become a practitioner of this method is marketed largely towards personal trainers.
And while there is a large variation in the experience and qualifications of different personal trainers, there is no doubt that the ability to assess a client’s hormone levels, and the interaction of these hormones with nutrition, sleep, stress, and exercise levels, is well outside their scope of practice.
This scope of practice is very clear on what a personal trainer is not qualified to deliver:
- Nutritional advice outside of basic health information and nationally endorsed nutritional standards and guidelines
- Therapeutic treatment or independent exercise prescription
- Independent exercise prescription for high risk clients
- Diagnostic tests or procedures
- Sports coaching
- Psychological counselling
Diagnostic assessments and prescribing nutritional supplements are outside the personal trainer’s scope of practice.
To operate outside this scope of practice is to risk being found legally liable for any injury or mishap that might occur as a result of your training or advice.
There are personal trainers with extra qualifications (such as exercise science degrees) who may be able to operate more broadly than this scope of practice, but any analysis of a person’s hormone levels needs to be performed by a licensed medical practitioner.
Not a personal trainer. Not a strength & conditioning coach. Not an exercise physiologist. Not a nutritionist. Not any number of professionals who may be concerned with the health and well-being of their clients.
An important part of any professional’s knowledge is the understanding of where the boundaries of this knowledge and expertise lie, and when they need to refer the client to a more appropriate health professional.
For this reason, I have largely avoided addressing the specific claims made about hormones and body fat distribution here, preferring to trust the opinions of those more qualified.
It’s important to note that if any of these claims turn out to be correct (that is, they repeatedly stand up to the scrutiny of the scientific community), it would be a game changer!
Take home message
You probably can lose fat from your trouble spots, but it may not happen in the order that you hoped!
There are no shortcuts, and it doesn’t look like any will emerge in the near future.
I would love to be able to tell a client: “yes, you CAN reduce body fat from the exact areas you want. It’s easy!” But I can’t.
Unfortunately, there are no shortcuts. It probably took years to accumulate that extra body fat and it may take months or years to lose it. Sorry!
Nick Jackson
Thursday 28th of February 2019
Just a comment regarding respect and decency about criticizing others. Mr. Poliquin was multilingual. English was not his first or second language. He is a native French speaker, learned German, and learned English - and has functional knowledge of other European languages. That is commendable, not something to be mocked at with comments irrelevant to the topic at hand such as, "complete with the author's spelling errors" as a jab at one's mistakes.
Learn how to be loving and charitable while taking issue with one's views. People will take you more serious I believe.
Silvana
Tuesday 3rd of April 2018
I have never found any spot reduction methods to have real results. I finally turned to laser therapy recommended by my dermatologist to reduce my last few stubborn areas. I am very pleased with the results and would recommend it to anyone.
Of course, regular exercise and healthy eating are required to keep the fat off, but that's not a problem as that is an integral part of my lifestyle. I power walk, power lift, and do power yoga to keep fit, strong, and flexible.
Dan Jolley
Wednesday 9th of November 2016
Hi James, I bring it up not to be topical, but because it is a modern take on an enduring misconception. It is a way of discussing spot reduction and a trainer's scope of practice in general, with Biosignature as a well-known example. I'm not aware of a more recent, well-known version of spot reduction, but if there is one I would be fascinated to look at it!
In your comments, you use the same rationale as Poliquin in his justification for Biosignature. Just because you observe poor sleep, and a skinfold measurement >10mm at the calf, does not mean there is a causal relationship between these two variables.
Ogi
Tuesday 1st of October 2019
I have a skinfold measure at the calf to be singificantly higher than 10mm, actually double, at 20mm...but I never had any sleep issues, nobig discrepancies in Circadian Rhytm, and also I am fairly lean with 11.8% BF, taken with DEXA scanning. So maybe I am exception to the rule, but this is how my body measurements are.
James Sebastian Roa
Tuesday 8th of November 2016
A compelling read, and to a fine degree I do agree with your argument. However, seeing that this method has been around for quite a long time, why only now bring it up? I myself was (am) qualified in doing biosignature and found that i didint buy into the supplement side of it but more used it as a marker and cross referenced it with a lifestyle planner ( circadian cycle, stress, etc) and found that it was consistent with set fat markers, the exception if medication or birth control was being used which would throw the markers off. Yes, it was defined as the be all and end all, and unfortunately nothing beats good sleep, good food, and deceant habits, however it does help identify signs of inbalance. Example, in 5 years I have never ever come across a person with a pinch of more than 10mm and above at the calves that had great sleep, it was so consistent. Make of that as you will. Again just curious as to why after so many years have you just written on this now.